
CDHD Tuberculosis (TB) Control Program
To ensure that local practices reflect current public health standards of care, Chelan-Douglas Health District provides tuberculosis consultation and oversight to local facilities and practitioners. TB Control Program oversight is provided by the CDHD Health officer, a contracted Medical TB Consultant, and the WA State Department of Health (WA DOH).
Program services are provided to residents of Chelan and Douglas counties regardless of ability to pay.
CDHD TB Control Program services include:
- In general, CDHD TB Control provides clinical care, case management, and direct observation therapy (DOT) for highly suspected and confirmed TB cases with intrathoracic (i.e., pulmonary, pleural, intrathoracic lymph nodes) involvement. Clinical care, case management, and DOT for extrathoracic TB cases are determined on a case-by-case basis.
- Contact investigation and treatment support for individuals exposed to active TB disease.
- Investigation of Class B individuals with suspected or diagnosed active pulmonary TB disease.
- Communications with primary care providers and CDHD TB Medical Consultant regarding case management and client status.
- Patient and family education as applicable to plan of care.
- WA State DOH reporting requirements and recordkeeping.
The CDHD TB Control Program does not provide:
- Laboratory services
- Latent or inactive TB Infection case management
- Extra-pulmonary TB disease case management (except on a case-by-case basis)
- TB screenings (e.g., no tuberculin skin tests, reading, or interpretation). For screening locations, see Where Do I Get a TB Test?
For questions regarding the CDHD TB Control Program, call 509-886-6400 ext 6456.
Active TB Disease: Diagnosis, Reporting, Medical Management
Providers practicing in WA State and hospitals are required to report suspected cases of active TB disease within one day (as soon as clinically suspected) to Chelan-Douglas Health District. (References: WA State TB Law Manual for Health Officers, RCW 70.28.010, WAC 246-101)
To report active TB disease call 509-886-6400 ext 6456
Additional contact information:
- Fax: 509-886-6478
- Mail (e.g., x-ray CD): Attention: TB Program, 200 Valley Mall Parkway, East Wenatchee, 98802
Note: Do not wait for culture confirmation to report suspect cases. Delayed reporting may increase transmission of infection.
Refer to:

Appendix I: Active Pulmonary TB Diagnostic Algorithm for Primary Care
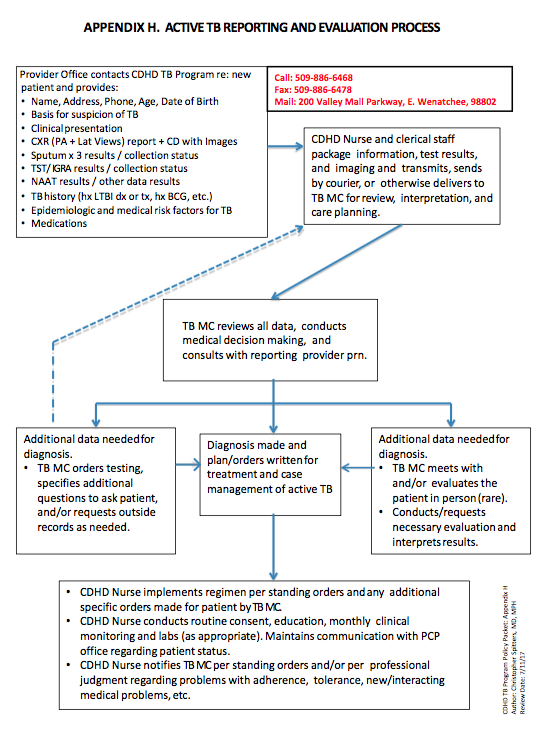
Appendix H: Active TB Reporting and Evaluation Process
Medical Management
- CDHD personnel will report all active TB disease cases to WA State DOH and the CDHD TB Medical Consultant. The TB Medical Consultant provides oversight to the CDHD TB Program.
- The patient’s primary care provider maintains oversight of the medical plan of care in collaboration with the CDHD TB Medical Consultant.
- CDHD requires the following medical information: lab reports, cytology reports, x-ray reports (both paper and images on CD), and progress notes. When applicable, health immigration records, healthcare power of attorney, and POLST Form. Because TB is a reportable disease, no patient release of information is required to share protected health information between CDHD and outpatient clinics or hospitals.
- CDHD personnel will contact the patient and initiate the TB plan of care.
- Active disease clients will be isolated in their place of residence until they are no longer infectious.
- Isolated clients visiting an outpatient clinic must mask (preferably before entering the clinic) and should be placed in an isolation room or at minimum removed from close contact with other patients.
Latent TB Infection: Diagnosis And Medical Management
Latent TB Infection is diagnosed and managed by a patient’s primary care provider (PCP) or Obstetrics Care Provider (OCP), in the outpatient clinic. Eligibility for any CDHD services related to LTBI is determined on a case-by-case basis based on CDHD Administrative Policy.
Latent TB Infection is not a reportable condition to CDHD or WA State DOH. (Note Exception: Immigration TB status (Class B). In cases of immigration, refer to Class B Evaluation Process. Appendix G: Class B Evaluation Process.
Refer to Latent TB guidelines: Primary Care Diagnostic Workup for Latent TB of Immunocompetent Patients.
Appendix E(1): Primary Care Diagnostic Workup for Latent TB of Immunocompetent Patients
Contact CDHD TB Program for additional policy detail.
Following LTBI diagnosis, providers should consider treatment for LTBI. Base the decision to treat and regime selection on all of the following:
- risk of progression from latent TB to active disease
- risk of adverse effects
- drug-drug interactions
- adherence potential and
- patient input
To calculate the risk of progression from latent TB to active disease, use the TST/IGRA 3D Interpreter. This tool estimates the risk of active tuberculosis for an adult tested with standard tuberculin (5 TU PPDS, or 2 TU RT-23) and/or a commercial IGRA.
Following LTBI diagnosis and decision to treat, refer to:
- Latent TB Infection Plan of Care Options: Appendix E(2): Latent TB Infection Plan of Care Options
- Standard Treatment of Latent TB Infection (LTBI): Appendix C: Standard Treatment of Latent TB Infection (LTBI).
- TB Drug Dosing Tables: Appendix D: TB Drug Dosing Tables
- Patient Medication Counseling Documentation Templates: Appendix K: Patient Medication Counseling Documentation Templates
Immigration Requirements
Refer to Class B Evaluation Process: Appendix G: Class B Evaluation Process
When this approach is not feasible, refer to the following recommendations:
Class B1 Pulmonary TB (active or inactive, treated or untreated)
- Obtain TB history
- Repeat PA chest radiograph
- If TST not done or <15mm AND patient not previously treated for active TB, collect blood for QFT
- Collect three sputum specimens if ANY of the following conditions are met:
- Visa examination sputum collection date was more than six months ago, OR
- Visa examination of sputum did not include culture, OR
- Visa examination did not include sputum collection
Class B2 Latent TB
- Dismiss if previously treated or not interested in treatment AND currently asymptomatic
- If not previously treated and interested in treatment:
- Obtain TB history
- Collect blood for QFT if TST <15mm AND age >24 months AND overseas chest radiograph reported as “normal”
- Repeat PA chest radiograph if overseas chest radiograph obtained greater than three months ago or not available AND TST>15mm OR IGRA positive OR age <5 years.
CDHD receives information from the WA State DOH about Chelan and Douglas County immigrants and refugees who were 1) classified overseas during the required medical examination process with a TB condition, and 2) who were instructed to obtain medical follow-up evaluation in the United States. The EDN document is used to collect information about these residents and to communicate with the WA State DOH and the CDC. CDHD compiles information, completes and submits the Electronic Disease Notification (EDN) TB Follow-up Worksheet to WA State DOH.
Immigration Resources
- CDC Immigration Requirements: Technical Instructions for Tuberculosis Screening and Treatment
- CDC: Immigrant and Refugee Health: Medical Examination FAQs
TB Diagnosis Classifications
Assignment Of TB Diagnosis Classification And General Approaches To Treatment
Class 0: Not recently exposed, not infected (or exposed > 8-10 weeks ago and infection ruled out with follow-up skin testing).
Class 1: Recently exposed (e.g., contact to a case of active TB), not infected (should become reclassified within 3 months).
Class 2: Latent infection (without disease). Positive reaction to the tuberculin skin test, no clinical or radiographic evidence of TB, and/or negative bacteriologic studies (if done).
Class 3: Confirmed active disease. Clinical, bacteriological, and/or radiographic evidence of current tuberculosis. This is established most definitively by isolation of M. tuberculosis.
Class 4: Old, inactive disease. History of episode(s) of TB, or abnormal but stable radiographic findings, positive reaction to the tuberculin skin test, negative bacteriologic studies (if done), and no clinical or radiographic evidence of current disease.
Class 5 High: Suspected active disease, diagnosis pending, with intention of empiric treatment (should be reclassified within 3 months).
Class 5 Low: Suspected active disease, empiric treatment not intended (should be reclassified within 3 months).
Per CDHD Standing Orders, the TB Medical Consultant will assign disease classification, order all treatment for active TB disease cases and maintain standing orders and care recommendations for LTBI management.
Medical management of class 1, 3, and 5 patients will be individualized but typically will reflect prevailing guidelines set forth by the American Thoracic Society, the Infectious Diseases Society of America, and the Centers for Disease Control and Prevention (CDC).
Patient Education
Refer to Patient Medication Counseling Documentation Templates for outpatient documentation recommendations:
CDC Stop TB Poster describes in simple steps and pictures how TB is spread and the difference between latent TB infection and TB disease.
Latent TB 12-Dose Regimen Instructions: Isoniazid and Rifapentine
Latent TB Medication Instructions: Isoniazid
Latent TB Medication Instructions: Rifampin
Latent TB Medication Instructions: Isoniazid and Rifapentine
Multidrug-Resistant Tuberculosis (MDR TB)
EthnoMED: Patient education tuberculosis resources in multiple languages.
Low Literacy Flip Book: What You Need to Know About Tuberculosis
Trends And Statistics
In 2016, there were 205 reported cases of active TB in Washington State and 3 in Chelan and Douglas counties. Of these cases, the majority were born outside of the United States, most often in Mexico, Vietnam, Philippines and India.
As latent TB infection is not routinely reported, the number of cases in WA State and Chelan and Douglas counties is not known.
- WA State DOH Tuberculosis Fact Sheet (2016)
- WA State DOH Tuberculosis Infographic (2016)
- WA State Communicable Disease Monthly Surveillance Summaries by County
- WA State DOH Communicable Disease Report (2015)
Resources
- WA State DOH Provider Materials
- Printable tools include Adult TB Risk Assessment, Pediatric TB Risk Assessment, Drug Regimens for Treatment of Latent TB Infection, Tuberculosis Symptom Screening, and TB Laboratory Diagnostics Summary.
- Drug-Resistant Tuberculosis: A Survival Guide for Clinicians
- CDC: Division of Tuberculosis Elimination
- Includes Tuberculosis Guidelines, online ordering system for educational materials, self-paced interactive TB study modules and epidemiological reports.
- Curry International Tuberculosis Center
- One of five Regional Tuberculosis Training and Medical Consultation Centers (RTMCC) funded by the Division of Tuberculosis Elimination of the CDC.
- Official American Thoracic Society/Infectious Disease Society of America/Centers of Disease Control and Prevention Clinical Practice Guidelines: Diagnosis of Tuberculosis in Adults and Children
- Official American Thoracic Society/Infectious Disease Society of America/Centers of Disease Control and Prevention Clinical Practice Guidelines: Treatment of Drug-Susceptible Tuberculosis
- World Health Organization TB: International epidemiological reports, TB fact sheets, and information on how to advocate for strengthening the fight against TB.
Continuing Education
- CDC: Core Curriculum on Tuberculosis: What the Clinician Should Know
- A self-study guide and reference manual for clinicians and other health professionals caring for people with or at high risk for TB disease or infection. Available in print and interactive forms.
- CDC: Self-Study Modules on Tuberculosis
- Nine self-study modules separated into 2 courses. CME, CNE, CEU, and CECH credits are available on successful course completion through the CDC.




